Two months ago, my mother, who has dementia, fell. The memory care facility called me and I rushed over; by then the parademics were getting ready to load her onto a gurney. I can’t describe that moment yet.
And here is where I say Mom is still alive and back in the memory care unit with her repaired hip. And I’m not really okay, but here is today, and there is tomorrow, and that’s what I focus on.
But this is about the hospital. What I learned during my mother’s stay is that ERs and ICUs are ill-prepared to provide consistent care-based treatment for dementia patients. Individual nurses were incredible. Gods, really. The woman who prepped my mom for surgery understood to speak slowly but not necessarily SHOUT, because my mother is not hard of hearing, she has a serious cognitive impairment. Prep nurse: god. After the surgery, my mother encountered a range of nurses, aides, social workers, doctors, and physical and occupational therapists, and each of them approached her differently and with variable levels of understanding. The PT who kept shouting into my mom’s face, “What’s your name? Can you tell me your name?” was not helping anyone. This is what I mean by “consistent.”
In her book Dementia Reimagined, medical ethicist and psychiatrist Dr. Tia Powell writes of the divide between psychiatry and neurology in treating dementia. The lingering stigma of the psychiatric approach to the disease has to do with the way sufferers were lumped together with psychotics, the deeply depressed, and the manic, when dementia was considered early in the twentieth century to be a “functional” disorder, having no discernable physiological source. The responsibility shifted to neurology as the brain was understood better, understood as an “organic” disorder. But because of that shift, Powell says, there hasn’t been enough consideration of what psychological functioning exists in dementia patients. What joy can still be found. What suffering can be prevented. It shouldn’t be an either/or proposition. “Dementia is a brain illness,” Powell writes, and what its sufferers need is the best care from both sides of the medical aisle.
This may be one reason why our society takes a “cure” approach to dementia and has generally marginalized “care” for dementia patients–including within the medical community. In other words, as dementia treatment has been taken over by neurologists and the medical research field, psychiatric care is no longer considered as much as it should be. I don’t remember that Powell makes that this correlation explicit, though the entirety of her book is about reemphasizing care. But she does mention numerous examples of doctors–specialists, in particular–failing to guide families through care-based decisions. Doctors are more likely to recommend another procedure, another treatment, another drug, and to do so without asking, “Is this making the patient’s suffering worse or is it relieving their suffering?”
This isn’t to say all psychiatrists excel at care, or that they do not overprescribe medication. But we do not talk about cures for mental illness like we do for dementia. Dignosed fifteen years ago with depression and anxiety, I have never been told to hold out hope for a cure. I’ve been told to learn how to manage the disease and how to ask for help. The emphasis has always been on care. (And I’m grateful for that.)
In the present moment of this soul-sick nation, as young White men armed with assault rifles massacre Black grocery shoppers in Buffalo and predominantly Latinx-American children in a small Texas town, the cure v. care dialectic is one way to judge the nation’s priorities, its values. Republicans insist there’s no “cure” for these slaughters, none that involves gun reform. They twist in the wind pointing at other so-called solutions that have no basis in fact; they say we ought to care for people with mental illness and in the process demonize them; they condemn video games as a prelude to violence when no study has ever determined a correlation; they blabber on about “family culture” and “the culture of fatherlessness”; and they propose arming teachers and building our schools into fortresses. When you dig through to the reality of their stance–that gun ownership rights are sacred (and profitable) and more valuable than people’s lives, including the lives of children–what you find is a perverse kind of “care” approach: There is nothing we can do to stop this “virus” of mass shootings, so we offer our “thoughts and prayers” and point to other red herrings. This kind of “caring” is, in fact, its opposite.
On the left and the “alt-right” (which is to say the fervently White supremacist/nationalist community), accelerationism can be accused of the opposite: valuing the cure more than care. Accelerationism is described as speeding the rate of social deterioration which will supposedly end in an eventual “cure”–for Marxists, post-capitalism, and for White nationalists, a White ethno-state–that will provide better “care.” Of course, a White ethno-state is no kind of cure, and as far as “care,” it can only result in genocide. Neither do I think Mark Fisher, who often gets associated with leftist accelerationism, ignored the importance of care, real care. If you’ve read his work, that should be obvious.
Maybe I shouldn’t bring Powell’s book about dementia into this political miasma, but she outlines a masculinist heroic thinking of medicine’s cure-based approach that undoubtedly echoes the cultural underpinnings of accelerationist thinking. “The dream of cure,” she writes, “can push care to the lowest rung of the ladder.” Politically, I hear the “Bernie Bros” in 2016, or Zizek saying he would’ve voted for Trump so as to push along society’s collapse and a subsequent revolution. To make that choice is to condemn thousands, millions, to greater suffering and death. Those condemned are already more likely to be at the lowest rung of the social ladder, living with various kinds of precarity: the poor, the disabled, Black folks, queer folks, trans folks, women, the elderly, children. That is not up for debate in 2022. We’ve seen it happening every day if we’ve bothered to look.
And for those who need caregiving: who provides it? As Powell points out, even today, “care” is too often seen as feminine work in the healthcare industry. In my mother’s memory care unit, every single nurse and aide is Black, most are of Caribbean or African descent, and all but one are women. They are working class, and having seen what I’ve seen, they are not paid enough for their labor. When they step outside that building, they’re confronted by White supremacy, and though I’ve never witnessed it, no doubt it seeps into the building, as well. The Trump administration’s dismissive and incompetent response to the pandemic made their lives hell, too. When we marginalize the most vulnerable, we also marginalize the people who care for them.
Care is supposed to reduce suffering and pain. Care requires listening, empathy, time, and resources. But in a culture that operates by a scarcity/surplus equation and thus a politics of expendability, care is not truly valued. How could it be? Care is not fundamentally productive, and under capitalism, expenditure must generate a valued return. Thus, we make it pay off. We claim scarcity–that money is needed for a new stadium, after all–to invent profit. The capitalists who make bank from the medical industry and healthcare system in this country, including the corporations who own assisted living and memory care facilities, demonstrate this system quite well. The suffering of others can be lucrative. But this wouldn’t be the norm without a politics of expendability, particularly where mental illness and elder care intersect with marginalized populations that are seen as a cultural and biological surplus.
To care is to make a choice. It isn’t “thoughts and prayers,” it’s action. It’s an ethical decision, and this may be why so many gravitate toward a “cure.” I’m not saying the search for a cure to a horrible illness like dementia isn’t crucial. Of course it is. But you and I can do precious little to find a cure except donate money and participate in clinical studies. And, yes, those are important. But how often do we donate money to organizations that care for the elderly who suffer from dementia? And how many of our tax dollars help fund such organizations?
We race for cures, we bicycle for cures, we swim for cures.
We do none of that for caring.
When we choose the cure at the expense of care, at least as it pertains to healthcare and disease, we ought to ask if we’re not giving ourselves an easier ethical decision to make. Supporting the pursuit of a cure feels heroic, and that alone, that emotional gratification, is a more immediate reward than the tireless, back and forth, one-step-forward-two-steps-back experience of caregiving, especially for patients with terminal and cruel, cruel diseases.
Ultimately all I can say at this juncture is that we would benefit from paying more attention to the “cure or care” dialectic, firstly because, as rhetoric and concepts, those words can be slippery. When we finally get hold of them, they can expose all the ways we’re failing as a nation. But it’s also because, as Powell writes, “We do not need science or compassion, but always both. … We need care and cure.”
~
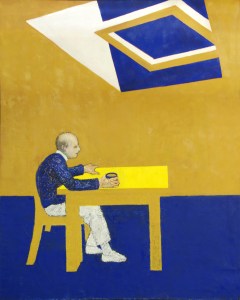
Note: William Utermohlen was a Philadelphia-born painter who moved to London in 1962. Diagnosed with Alzheimer’s disease in 1995, he continued painting. Blue Skies (pictured above) was his “last large scale painting” according to these notes about an exhibition of his work at Loyola University Museum of Art. You can visit that page for more examples of his work.
